 Dr. Angela Haczku is a professor of medicine here at UC Davis School of Medicine and she is an internationally recognized expert in pulmonary immunology. She is the director of the UC Davis Lung Center and associate Dean of translational research for the school of medicine. She has been amazingly connected to the UC Davis health work with COVID-19 and she is the co-author on a paper describing the first patient in the US to get the disease through community transmission. Dr. Haczku is also involved in clinical trials of treatments and diagnostic tools that are being developed at UC Davis for COVID-19 and she gives us a tour of all those efforts. It's quite impressive. *Introduction of Dr. Haczku above was done by Dr. Mark Winey, the Dean of UC Davis College of Biological Sciences. Dr. Angela Haczku Town Hall video with English and Spanish subtitles can be found here. In addition, a summary of this Town Hall, including student questions, can be found on this Twitter thread. Transcript of Dr. Angela Haczku's talk First case of community acquired COVID-19 It's very interesting because it's like a medical mystery. There was this cold like symptoms that was in late February. This is sort of the peak of flu season and she went to one of the hospitals and her condition worsened and they decided to transfer her to UC Davis. At UC Davis they had to incubate her and put her in the Intensive Care Unit and started to figure out what was wrong with her. She had pneumonia and they tested her for flu and other infectious possibilities but everything came back negative. And by that time mid to late February doctors were suspecting that it might be enigmatic Coronavirus disease, that the media was talking about from China. But this patient had zero connection to China. And because of this, she didn't have the criteria for testing. I have to tell you that at that time, 20 test kits were available for the entire county, entire Sacramento county, so the CDC had a very strict criteria to be able to use one of these test kits. But the patient's condition kept getting worse and it became life threatening and the team of our doctors insisted that the patient be tested for COVID-19, and finally CDC agreed and got the patient’s blood for testing and it turned out to be positive. And with that they immediately had to change the testing criteria because it became evident that a person didn't need to have to come in contact with obviously infected people and that community spreading of this disease was possible. And by community spreading you can imagine that asymptomatic people can also transmit it and they could be infected and it's not really obvious who is infectious and who is not infectious. So not only did the testing criteria were flexed at that time but the FDA also allowed in house testing to be performed in hospitals. So, what we did here, at UC Davis, we had the viral isolate from the patient, and that was done over the Davis hospital, and was sent to a BSL-3 facility where it was put into culture to grow. And then the virus it was yours for developing testing and that allowed much more people more suspected patients to be tested and then later on that procedure was set up. And then UC Davis bought an automated system from Roche and because of that new system now thousands of samples could be tested daily. So because of this patients disease and how the diagnosis was figured out, not only the CDC flexed its rules but at the same time the FDA allowed population testing using in house testing kits. So the government had strict test kit rules for a lock down people and ordered a shelter in place situation which is actually, as you know, here in effect. And this is to avoid what in other countries has happened, especially in Italy, where lots and lots of people got sick a lot a lot of people have died. And this is the scary nature of an epidemic and in fact this epidemic became a pandemic because every country in the world got affected because of the highly contagious nature of the virus. Here (below) I have a conversation with Governor Newsom, who brought up six criteria for lifting this draconian shelter in place ordinance and amongst those we have to have the ability to monitor and protect the community to testing, the ability to prevent infection in people who are at risk and the ability to develop therapeutics. Those three highlighted points were there because this is what we use at the School of Medicine and the entire UC Davis to address this viral situation. 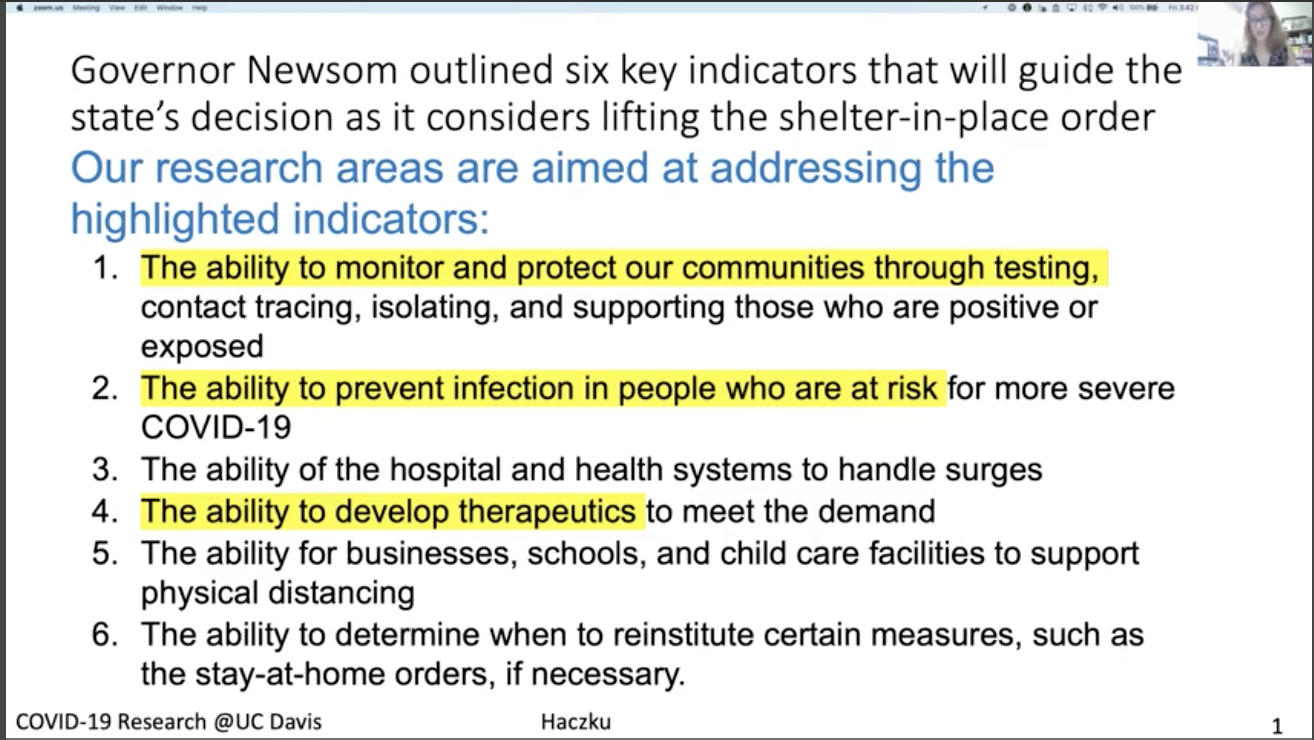 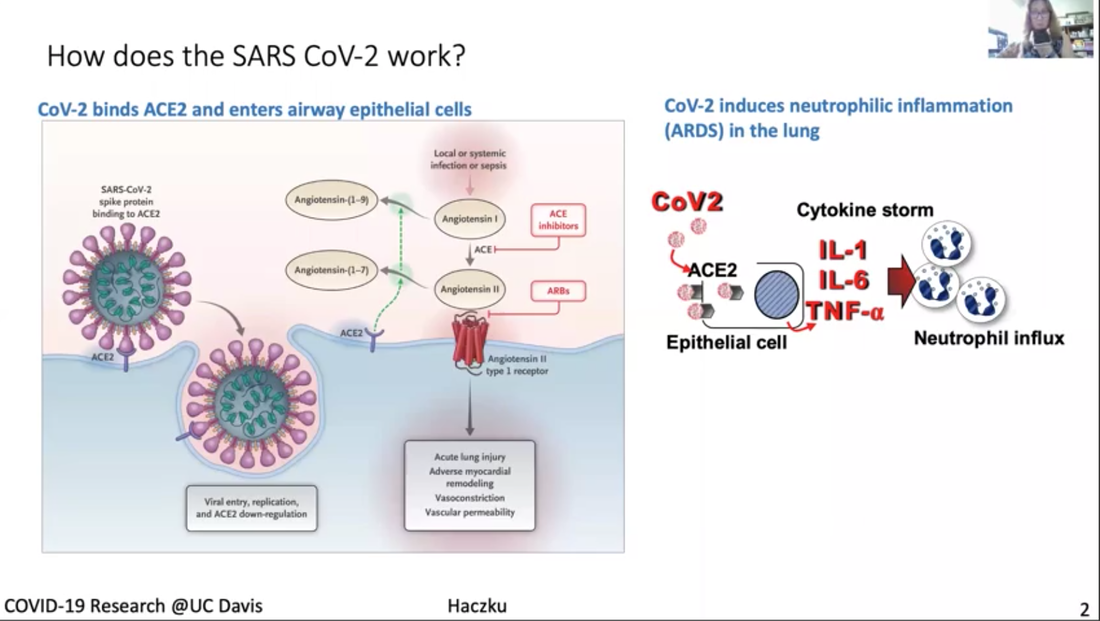 First, I would like to explain a little bit, how this corona virus work (figure above). Third I don't know if you can see my cursor, but if not then can you see this bean like little creature, actually two of them in the picture, and it engages with this ACE2 molecule that is sticking out from a cell membrane. This is the picture of the cell and a cell membrane. ACE2 is an enzyme, its angiotensin converting enzyme 2 and it happens to be specific, and if the enzyme is expressed on the surface of this cell and it happens to be an airway epithelial cell it helps to internalize the virus. It's like the Angiotensin is this Trojan horse. Once this is inside a cell, it will harness the cellular nuclear transcription and translation. And then these cells not only multiply inside the host cells but it destroys those cells. So, as a final cry for help, these dying epithelial cells release a cytokine storm. And this cytokine storm is a double-edged sword because the heightened inflammation might help eliminating the virus, but at the same time it also destroys the lungs and often it results in a fate called acute respiratory distress syndrome, ARDSs. ARDS is 50% lethal and it is caused by the influx of these neutrophilic granulocytes from the circulation into the lungs that will kill your respiratory system. 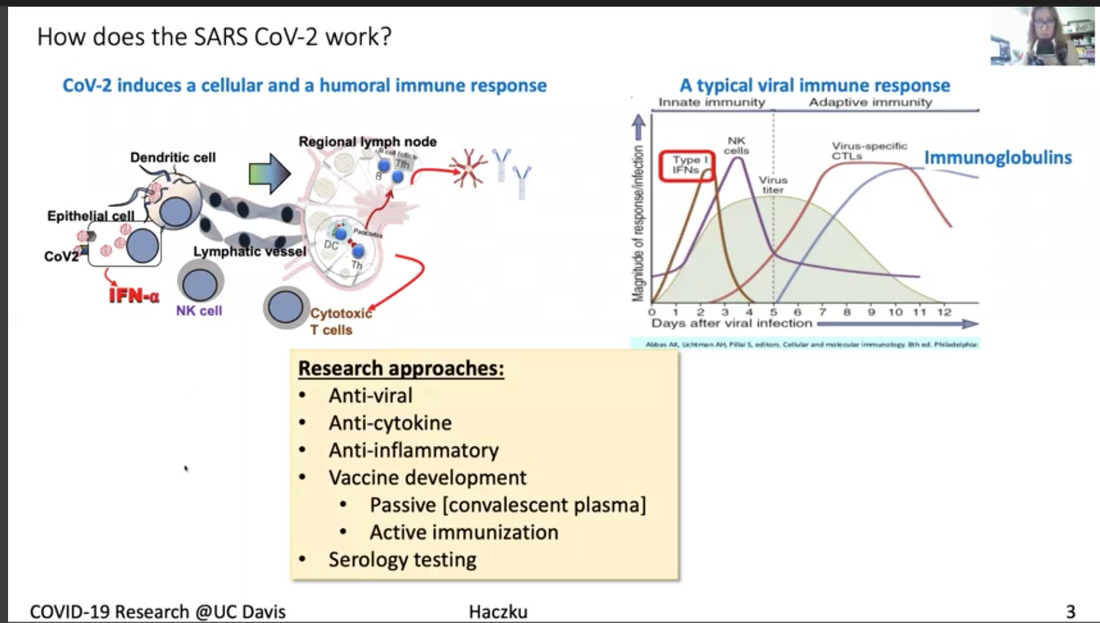 Description for the figure above. The virus not only destroys the area but activates the immune system, boost the immune system which is represented here by dendritic cells, and the other system, including the T lymphocytes and the B lymphocytes. Activation of B lymphocytes will result in production of immunoglobulin. These immunoglobulins, you can see here in this graph on the right-hand side are represented by this blue line their production comes up then the viral titer goes down. So as you are getting better and recovering from the virus your number of immunoglobulins increases. This procedure is harnessed by vaccine development efforts. The entire system of how the coronavirus works has these steps that I described and each of them could be targeted by therapeutic efforts. One area is to target the virus itself. These are called anti-viral. And one of those is remdesivir, the drug you may have heard from the news. We also, as soon as our patient was diagnosed with COVID-19 we received remdesivir from Gilead overnight and gave it to the patient who got better. Apparently it looks like that remdesivir works by inhibiting Coronavirus, so it's a good therapeutic. We can also target the cytokine storm by inhibiting it so it won't kill our lungs using anti-cytokine effort. And also we take anti-inflammatories, you all know that you take Tylenol or ibuprofen when you have fever during a viral infection. We are putting a lot of effort to develop vaccines. At the moment anti-coronavirus vaccines are not available and it might take quite a long time to have something that is actually working and it is protective. What we need to do is to develop very good detection system or serology that will detect these immunoglobulins I showed you here represented by the blue lines in the graph. 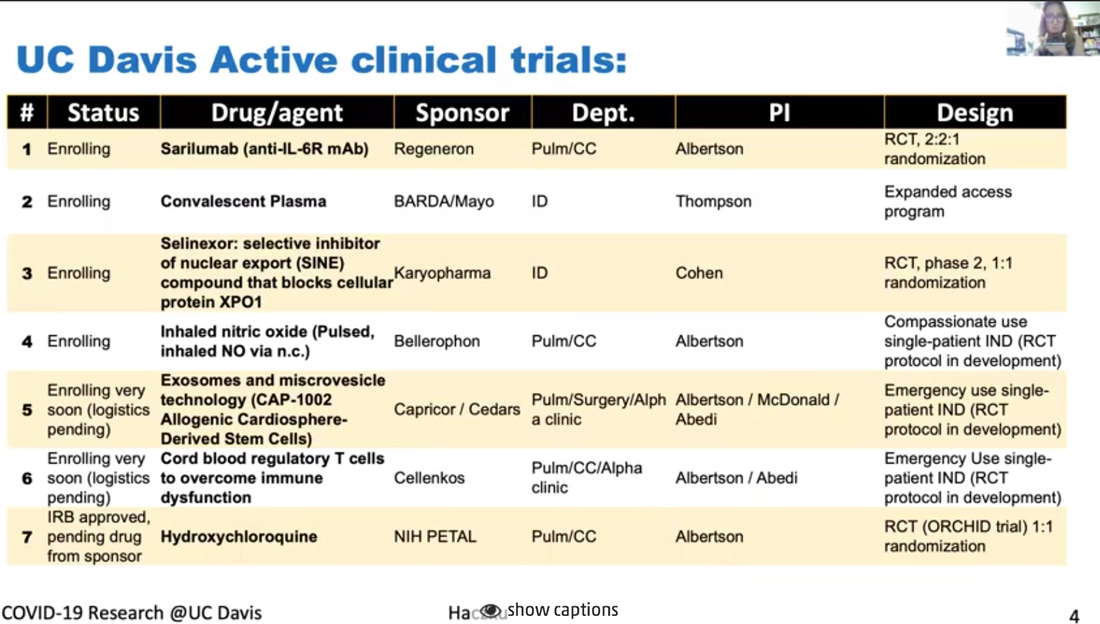 This is a list (above) of ongoing clinical trials that we have here at UC Davis in the ICU, one of them is an anti IL monoclonal antibody called sarilumab, and this targets the cytokines storm as I explained. Another one is convalescent plasma, it gives patients those immunoglobulins from other people who already recovered from the viral infection because these immunoglobulins are thought to be protective. Another one is another anti-viral drug called selinexor, it inhibits the viral transport inside the cell. Another drug is inhaled nitric oxide, it's been shown to have anti viral effects probably because it's an oxidative stress radical. There are STEM cells and STEM cell derived exosomes and microvesicles that have shown to have anti-inflammatory effects. Also cord blood derived regulatory T lymphocytes, which are suppressing the hyper immune activities. Lastly, you probably heard from the media about hydroxychloroquine and now it is being tested in a proper clinical trial. 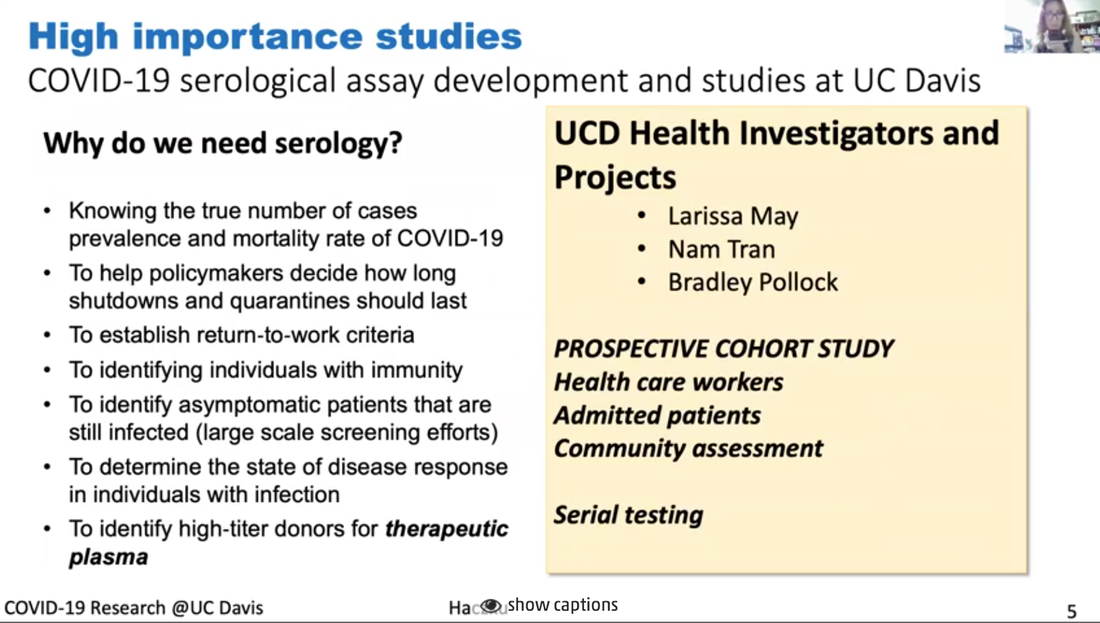 I just singled out a couple of studies here (figure above). And just wanted to stress again that serology, that is the detection of the immunoglobulins, is a very important part of determining whether a person has infection, whether the person has undergone the infection and developed immunity and whether the person who is being vaccinated would respond to the vaccine, with protective immunity. We have a number of arms to this study here at UC Davis. 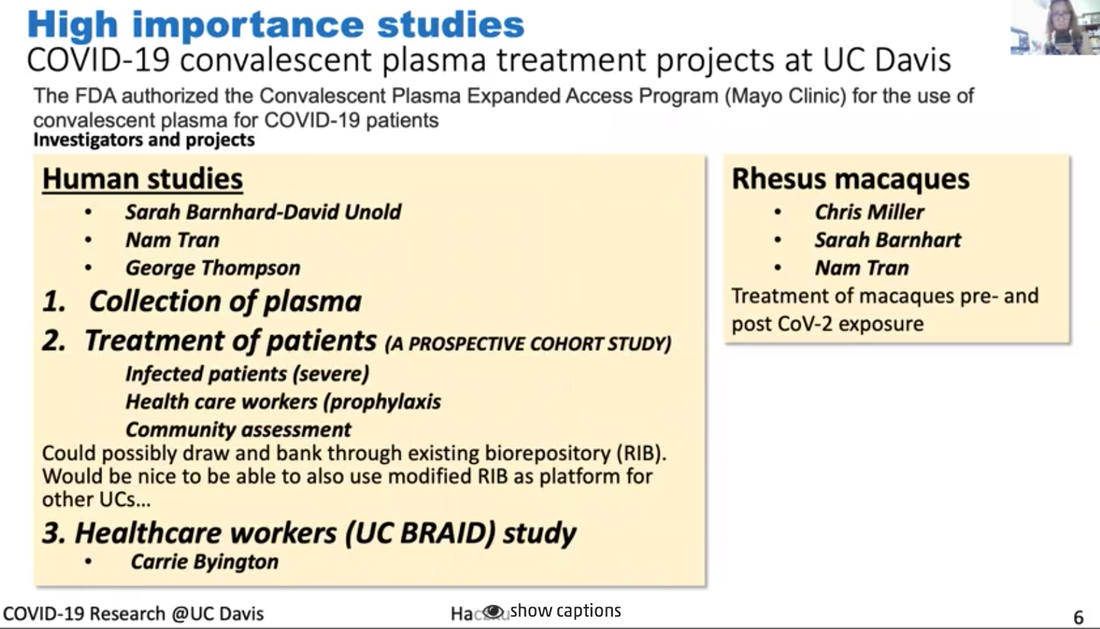 I mentioned the use of these immunoglobulins that we can take from patients who already recovered from the viral infection and after recovery their serum or plasma which contains these protective immunoglobulins, and this plasma treatment was approved by the FDA quite early on to treat severe patients who would have no other choice, no other treatment choice. And we have currently a trial going on there. It's called in a compassionate manner. These patients in the ICU can receive convalescent plasma, but we also have a study in which we infect the rhesus macaque with coronavirus, these macaques are also susceptible to the virus and we will test whether indeed convalescent plasma would protect the animals from severe disease (see figure above). 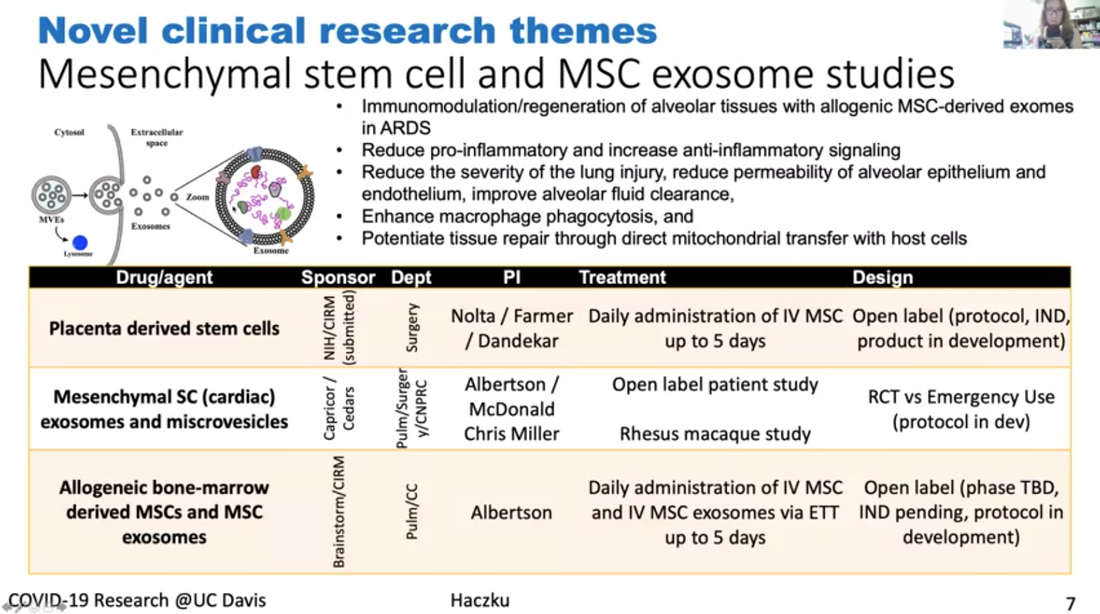 Lastly, I wanted to mention this study or these studies (figure above) we have actually several of them ongoing using the mesenchymal derived stem cells and stem cells derived micro vesicles or exosomes. It was shown that these stem cells not only reduce pro inflammatory processes and increase anti-inflammatory signaling, but they can reduce the damage that is done to the respiratory epithelium and also the blood vessel endothelium. They can have helpful immune and hunting effects on the macrophages. They can enhance macrophage phagocytosis. Phagocytosis is very important to take away damaged cells as well as to take away the viral particles. And through some mechanism it was shown that these stem cells and stem cell derived particles enhance the repair process that needs to go on to restore the tissue homeostasis after inflammation caused by viral infection. So, we have three of these trials going on at the moment. Hopefully these trials will result in some new discoveries and some of the treatments will prove to be useful. Remdesivir amongst them has already undergone a rigorous trial and has shown some beneficial effects. So that's one option for very severely affected patients. But at the moment our best option is to stay locked down and remain sheltered in place until the infection is still a threat. Transcript of the questions from students Q: There are some questions that kind of revolve around the confusion between the idea that you wanted an immune response to protect you from a virus. But on the other hand there are issues with too much immune response. Can you maybe elaborate a little bit on that? I think the specific question had to do with IL-6 being an inflammatory cytokine. Why would you want to inhibit that? 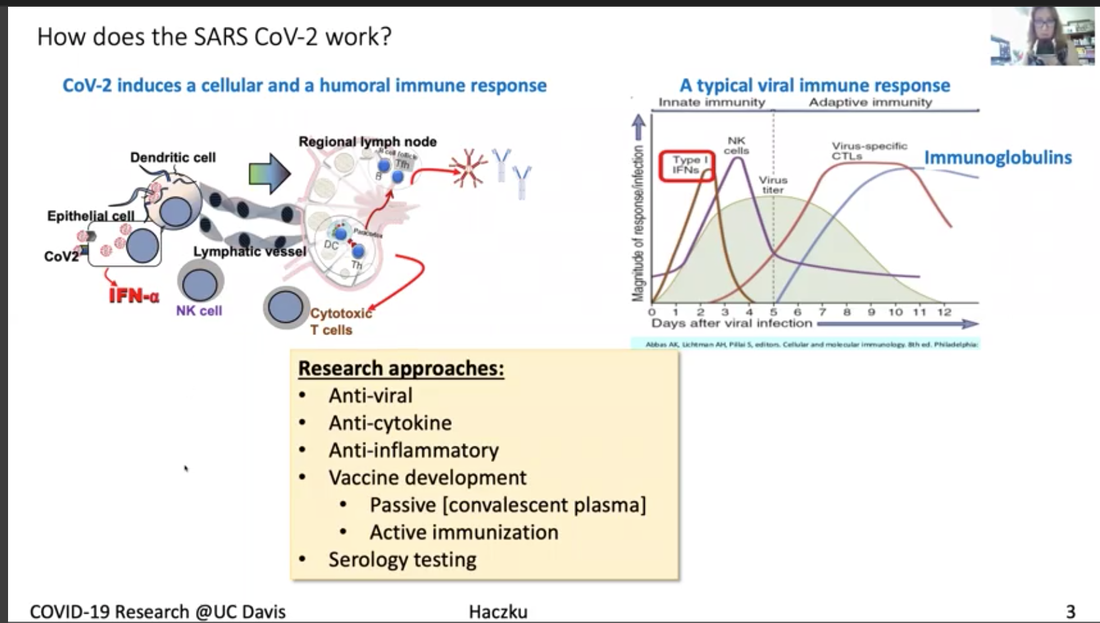 Right. I think it's all in the timing. IL-6 is released by highly activated immune cells, macrophages and dendritic cells, as well as epithelial cells. So, if you look at the left (figure above), left most spot shows the very early stage of the infection and in the timeline you see the first peak, it says type 1 interferon, which is interferon alpha and interferon beta. And those are very highly true inflammatory cytokines. And those are released by epithelial cells and innate immune cells including the dendritic cells. And that's necessary because these cytokines they alert the immune system, they wake it up it's like wake, wake, wake, you have to go to work and so the immune cells start to rush into the side of infection and they try to do their job. What that job is for the dendritic cells is to phagocytose, to pick up the particles and the dead part of the epithelial cell that contains the viral components. So, you know that all the proteins are built up of amino acids or smaller building blocks called peptides. And the way you educate your immune system is through presenting these antigenic peptides to T lymphocytes. So that process happened here in the regional lymph node. You can read I titled this little bean like structure here, this regional lymph node. When you have the viral infection and you touch your neck, you feel your regional lymph nodes swell up because they start working. What's happening in these lymph nodes is that dendritic cells present the antigen to T lymphocytes and T lymphocytes collaborate with B-lymphocytes to end up producing these immunoglobulins. And so this process is very highly promoted by IL-6. When an IL-6 is in the mixture you have a rapid production of immunoglobulins. So why would you want to inhibit this situation? I’m going to explain this with the figure above. Look at the cartoon that I put together, IL-6 is a central cytokine that promotes influx of neutrophilic granulocytes. Our blood is full of neutrophilic granulocytes at any time. If you look at the number of your white blood cells it's essential for our lives that we have about six to eight thousand cells per microliter, white blood cells per microliter. And half of this is all these granulocytes. So, it's inside us but what happens here when IL-6 is released in the lungs, these granulocytes are instructed to go into the lungs and what they do in response to leaving the circulation, they become extremely activated. Then they release their enzymes, those enzymes chew up the lung tissue, it's like World War II, but when you release these atomic bombs that's what these neutrophilic granulocytes do. They look very pretty when you just take them from the blood and they are mild and non-activated. But they become vicious once they are activated and they are the ones that can kill you. At the same time, they are also very important because under normal circumstances, if you prick your finger with a splinter and you get bacterial infection, or you get any kind of infection, these neutrophils come and they get rid of it. Under controlled circumstances these cells are very useful. You can think of them as good soldiers become bad when there is a virus like this. And then there is IL-6 around, it will craze them and it will make them extremely dangerous. To control that situation IL-6 can be taken off of the equation and then you can make the inflammation more subdued. Q: Other questions related to that I think is why some patients don't they experience a cytokine storm? And there was a question about children who are being infected but obviously not getting the same symptoms. Is there some indicator that some patients are going to be more sensitive to the cytokine storm? Yes, I will say that there are a lot of different components to this system and it's not just whether you're more sensitive to the effect of IL-6. But whether you respond to the virus by a heightened inflammatory response. What we know about inflammation, and actually I can talk about inflammation for 24 hours straight or even longer, but just try to condense this into a short answer. Inflammation is important as I explained, we need to have the inflammatory response. Because that protect us from outside invaders, virus, bacteria, fungi, anything. However, under normal circumstances inflammation is stopped. There are mechanisms that amplify the inflammatory cascade those are called pro inflammatory steps including the release of IL-6 and there are a number of other cytokines, TNF alpha, IL-1 also chemokines, IL-8 it's very important, these are all released within minutes if not hours. Prostaglandins, leukotrienes, five minutes, you will get a surge of these. And these are pro inflammatory cascades. Once inflammation peaks, the anti-inflammatory mechanisms such as protective inflammation resolving molecules start to enter into the equation. What they do, they bind to the cells that release these mediators and they switch the release off. So I've being studying for like 15 years, surfactant protein D, it's one of these protective epithelial derived molecules that's released in our lungs. We are full of surfactant protein D in our system. When surfactant protein D is proper and is around it will turn off your inflammation and you will get very good viral elimination. Maybe you feel a little bit tired, a little bit sick, but after third day you are fine and you are back to work. Hyper inflammation happens, then you have a deficiency in these anti inflammatory mechanisms. So for example, if you have a mutation in one of these molecules, you have difficulty controlling inflammation. And it's actually a very interesting mechanism. For people it's difficult to imagine because you think, Oh inflammation comes and then it goes away. No, it doesn't go away it has to be actively suppressed and we have a wonderful built in process to do that. And molecules like TGF beta and IL-10 produced by these regulatory T lymphocytes, that are also used therapeutically, that I mentioned we have a clinical trial on that, those also suppress the inflammatory response. Q: Students were quite interested in the antibody the humoral response. How is COVID-19 presented? You were mentioning some of that as it gets inside of the cell. Is it going to endocytic compartment, which cells are presenting that virus? Is that known? And then sort of what are the most important antibodies? -Yes, dendritic cells present the virus. They are the professional antigen presenting cells and they are the ones that are very important. They express those receptors once they go build up these dying complexes with dead cells and viruses and once they're full and mature, they have a lot of these little receptors they are like the wheels on vehicles that propel them to go into our regional lymph nodes that they can actually present the antigens to the adaptive immune system to the T lymphocytes and up on this presentation, these T lymphocytes become very active and they start engaging the B lymphocytes and then B lymphocytes produce immunoglobulins and out of those, the most important one are IgG. All immunoglobulin production starts by germline switching and that combination, and IgM is the first one. And then that will turn into IgG in the presence of interferon gamma. So, IL-6 six interferon gamma promotes IgG production. Q: I guess part of the question I think they're asking too is, so how long does your immunoglobulin response last, after infection so in other words, how long would you be protected for? So maybe you can talk little bit about memory as well as IgG levels. You know that's the $60 million question. It's not the $60,000 it's $60 million or 600 million. I don't know, because some antigens, when you get immunized against it as a child, they last until you die. Your entire lifetime. Some antigens like influenza you have to get it every year because it lasts a season and then it's going to be a different one. What's the situation with Coronavirus? We don't know yet. And that is a really scary thing. Q: There was a question earlier on about using antibody therapeutics, so making either chimeric human antibodies. I think the question was addressing whether we could block entry into cells using some of the antibodies and using sort of monoclonal antibody technology. Is that something that you know is being explored or thought of at this point? The monoclonal antibodies, those are really wonderful but they are not the convalescent plasma kind of antibodies. The monoclonal antibodies are synthesized to target various components of the inflammatory cascade such as IL-6, which I already explained, right? But you can target other, like you can target IL-1 perhaps, you can target other very bad components that you don't want to get out of hand. So that's what the monoclonal antibodies do. Monoclonal mean that a particular antibody is capable of recognizing only a single chain of amino acid, a single peptide and that's the actual peptide that was used originally to immunize that T lymphocyte and the B lymphocytes. And that was done all in the Petri dish. It was called the cloning, you're cloning the exact same cell over and over and over again. Those are the B lymphocytes, they proliferate and they're producing this one single antibody. Naturally when you get the viral infection, this is not what happens. The immunoglobulin profile that the B lymphocytes produce, they target many different peptide components of the virus protein. I don't know what the molecular weight of the entire viral capsid and nucleus is, it's huge and it has many, many, many proteinaceous components that are used by our immune system to generate immunoglobulin against. So, when you have this convalescent plasma, the blood that you take out from people who went through the viral infection, it contains a mixture, very wide variety of immunoglobulins, and this mixture of immunoglobulins can work very well because these immunoglobulins can latch into a lot of different parts of the virus. And what this mechanism does it helps mopping up the viral particles and the virus by phagocytic cells such as macrophages and the dendritic cells. And they help mopping up, clearing out and eliminate these viruses, so that's how convalescent plasma works. Q: I don't know if I did justice to the student’s question. This student had asked because of some information we had heard about the reservoir hosts, the animals that hosted the Coronavirus to begin with being immune. I think the question was really about whether we could take advantage of their monoclonal or their antibodies to generate therapeutic antibodies, which seems like a cool idea, but maybe not one that's easy to tackle right away. That's another $60 million question but I think it would circle back to my explanation about the natural built in protective anti-inflammatory pro host defense mechanisms. So just imagine that... I’ve been studying chronic inflammatory diseases such as Asthma and COPD, and what these diseases teach us is that we have to have a well toned, well muscled immune system. It's a little bit like you go into the gym and maintain, it helps your general health, you feel better, you're stronger, you're less prone to break downs and so on and so forth. The same with the immune system. So, as the immune system ages or you have other comorbidities like diabetes, obesity, that are all detrimental to your immune system, you will get two kinds of impairments on the immune system. On the one hand your immune system loses its edge to take care of foreign invaders. Which is done by phagocytosis and in the mucosal surfaces that you get exposed to. And on the other hand, you lose the immune system's ability to produce these anti-inflammatory molecules so every time you get a small infection you will get a huge inflammatory response. So that can naturally occur as we age so you're always more hyper inflammatory and more susceptible to infection. If you're a younger your immune system is also stronger and probably that have an iron strong immune system. That's why they can harbor the virus but not get sick from it. And also it’s a philosophic thing, because this is how viruses and infectious agents survive. They don't kill their host. It's like a scary sci-fi movie. They keep them alive, okay. So just imagine if corona virus would be so deadly they would kill every living creature and the entire humankind. It would be... The virus would shoot itself in the foot. They don't want that. The virus needs the host to stay alive. And it's not just, there are a lot of parasitic creatures that need us to stay alive. In fact, we don't call them parasitic creatures. We have approximately 100 trillion microbes living inside us. At all times, 100 trillion, you are full of it. I highly recommend if you have the chance once to do a swabbing in your mouth and put it on a slide, stain it and look it under the microscope. You will be horrified because it's a swamp. We have a living swamp in our mouth, all over, in the eyes, ears, everywhere, we're full of it. So, you see these creatures lives inside of us lives with us and I would say we need them too because often they are the ones that keep the immune system always on its toes. It's like a little bit of a tug of war, between the foreign creatures and the immune police and if they have a good balance then peace is there. And if the balance is upset by something, I don't know, you're getting the nervous breakdown in a stressful situation and then you break out on your skin, you start to have diarrhea and stomachache and that sort of thing. It's all because your immune system and your microbiome is starting to get out of control. So yes, unfortunately in these trans species creatures, they are not at all accustomed to a creature like this, CoV-2, SARS-CoV-2 and that's why it hits some people very, very badly. Sorry, this was again a long explanation, but I hope you understood it. I don't know. But you can probably shout and if you didn't understand I would be happy to explain it better or more. Q: The student was asking about whether a subsequent infection, so if you were infected and then were re infected, will it be mild or serious? I guess it's kind of like the influenza case, would you need to have any sense of that? What's your perspective? First of all just remember we never, humankind has never had a coronavirus pandemic before. We had flu pandemics and we get the seasonal flu, coronavirus never. And this was the first season with coronavirus. So, my answer to this is no. I mean, I don't know. I don't know if you were... If you got this, this time, if you will be protected the next time, I don't know. Sometimes when you are infected with the common cold and coronavirus also is responsible, a different kind of Coronavirus is responsible for the common cold. You can get it at the beginning of the winter, and then next time at the end of the winter, so twice, there is no immunity there. For flu, there is a partial immunity, which is interesting. And it's also scary because we've been developing vaccines against the flu for like 25 or 30 years now. Yeah, and it's, you know, not really perfect. Sometimes it works, sometimes it doesn't work at all. And so we don't know what we are doing. And by we I mean immunologists in general. But maybe there are some experts who have better ideas and actually at UC Davis coronaviruses were studied and there is this professor, Niels Pedersen and he studied Coronaviruses for 50 years, for his entire career in cats, and he actually was investigating a lethal cat disease that's caused by a Corona virus similar to this coronavirus. And a few years ago, he was the one who tried out remdesivir that antiviral drug and they figured out that it actually cured this deadly cat disease almost all of his cats in that clinical trial got better after remdesivir and at that time they were using remdesivir for Ebola trying to treat Ebola with it but it didn't work at all. Researchers in China used rhesus macaques and read his paper and they decided to try out remdesivir and they were very surprised to see that remdesivir made the monkeys better and that was last December and Gilead immediately started to develop it into clinical trials. They did have a lot of it left over from the Ebola and that's why they were able to launch a lot of clinical trials to look at the patients. And one of the first months came down just a few days ago when Anthony Fauci announced that it was positive so it's working. Other than this, we don't know if you get immune, we don't know, maybe convalescent plasma, maybe that, but we don't know that either. Some people were asking about the ACE2, and ACE2 is expressed everywhere. And that's a very good question because I was thinking about that too. It's expressed everywhere and yet Coronavirus comes in through our respiratory tract. Even if you if you get a coronavirus into your GI tract, it's an oral fecal infection. In fact, it attacks your respiratory tract. So that's a very good observation and I don't know why that is, yes, it would be nice to know. Q: I assume it's true that other corona viruses are also using ACE2 to gain entry into cells? Yes and not just corona viruses but even influenza. And then there is another receptor it's called TMPRSS, you guys can look that up too, that's a similar one. And TMPRSS and ACE2 they also work together. These are the two known receptors for SARS-CoV-2. But they are not exclusive they might engage other viral particles too. So that's how we evolved... I don't know why nature allows that us, poor mammalian creatures can have viruses attacking us. I'm not really sure what's the purpose of that and it sucks, but that's the way it is. I think we are lucky that this Coronavirus didn't just kill the entire human kind, it could have, but it didn't. Not yet at least. Q: Maybe virologists and immunologists are not sure yet but I was just curious whether some of the connection to ACE2 had to do with its own sort of cell physiology that it's connected to proteases inside the cell that are important for releasing it. I wonder if that had something to do with the viral life cycle. I know there's been some papers sort of hinting at that, but I was wondering what your perspective is. In order for the virus to get entry, it needs to be cleaved off from the part that's engaged to the enzyme. So it's the actual site that caught the virus and then it can get into the cell. So yes, unfortunately this is enzyme function and some of our enzyme just some of these viruses hijacked these human enzymes and human processes to attack us and to make them sad, invisible for the immune system. So as soon as a virus infect a cell, it becomes... As long as the cell is alive, it becomes hidden from the immune system because immune cells, when they survey the area, they only survey outside it's like little bit like the police when they are walking up and down the street, they can only see what’s outside, they cannot see what's going on inside the house. And so that's the same with the virus. However, the immune system developed two cell types. One is the CD8 T lymphocytes which has the MHC class one recognition part, the CD8 and what it can do, it can actually recognize the MHC class one on the viral infected cells. It's a little bit like an alarm. A "help me" system that when the virus infects the cell it express MHC class one and basically that's a death sentence because these T cells are cytotoxic and then the other cells up is the natural killer cells and those natural killer cells are also designed to come and kill the viral infected cells. These two cell types we have protect us from viruses that are inside ourselves, but the way they work is they kill those cells. So, it's too bad for the infected cells. Q: I wanted to ask you a little bit about this idea between the two kind of pathways to therapeutics. Obviously, there's talk about developing vaccines and antivirals to stop viruses and stop infections or reduce them. On the other hand, there is this sort of anti-inflammatory approach and so I'm wondering how you view the balance between those two paths, are they something we should be pursuing sort of with equal vigor for both or is there a priority here? In terms of research we do a lot of anti-inflammatories I don't mean we but I mean humankind, we have a lot of anti-inflammatory drugs. So those drugs can be repurposed to treat if you would get an out of control inflammation during viral infections. In regards to antiviral approaches, the experience with Coronavirus, with the... for example, remdesivir very clearly shows that a viral specific approach, unfortunately, nothing is easy. You have to work out a viral specific approach. Remdesivir appears to be specific for this SARS CoV-2. I don't know somebody asked whether it works for the original SARS as well, I can't remember but originally, I think they found it worked on some corona viruses, maybe in vitro, but unfortunately it didn't work for Ebola, which is also a corona virus. So, it looks like that this treatment even though they attack general viral biology still some viruses are more sensitive to this than others. Thus, I think it will require a lot of experimentation and to figure it out what would be the Achilles hill for the Coronavirus and then we have to seriously go for that. Moderator- So, the answer is take advantage of the drugs that we have already to try to reduce the impact on patients who are pursuing multiple approaches against the virus Yes, yes of course yeah but better to prevent the infection from happening. And so as much as it sucks to be locked down in solitary confinement and driving everyone crazy. Still, unfortunately that's the only way we have right now for prevention. And then of course social or physical distancing and use of mask and being very good about washing your hands and that sort of thing. And not touch common surfaces or wear gloves and that sort of thing. So you just, unfortunately, we have to be very conscious and very vigilant and very intentional about avoiding getting infected because you don't know ... With this virus, you don't know what would happen if you do get infected. It's not like there's some mild childhood disease their parents decide it's better to put the two kids together once one of them gets it so that they get over it at the same time. Because that will provide them with immunity and also it's mild, it won't kill them. But this one is actually very hard to predict. Back to our original patient... in flu, you know that under the age of two there is a high susceptibility and also over the age of 65, 70 people are very susceptible to flu. Looking at our statistics, every day we get sent by email from the hospital, it actually was disturbing that the 35 to 50 age range population was the most... Most of the patients came from that age range, not the over 65 age range. And then a child, I think there at least at UC Davis, there was only one child. But there were some children who were very severely affected also. So, our general assumptions for how infections and inflammation works in other cases might not be applicable to coronavirus disease and they need to learn a lot about this. Q: In your last answer you touched a little bit about the range of people who are affected and how they're affected. But how many patients have you seen? Have you seen some of the really unusual outcomes? Like there's been news stories about really odd strokes in middle aged people. So what's your, in the clinic experience been like? I am not a licensed physician. I am an MD by training, but I do not work in the ICU. So I do understand a little bit about what's going on and I can comment from that perspective, but not first-hand unfortunately. So yes, indeed a lot of the patients had coagulation and it's very disturbing because when you have the cytokines storm, and an inflammation that's out of hand it can actually engage the coagulation cascade as well. And in this situation then the coagulation cascade goes out of hand. Coagulation is also a very nice system. But it has to be induced. So, you probably know very well when you cut your skin and the blood comes out and then after a while the bleeding will stop and so this coagulation systems starts and then peaks and then has to be stopped. And then it has to be eliminated and it's a complex archaic cascade. Similarly to the compliment cascade. I didn't go into it but one way for the phagocytic cells to get activated by the immunoglobulins, is through activation of the compliment system. So both the compliment cascade get involved and the coagulation cascade, both of these involve a lot of proteins and it's like a chain reaction. So activation of one protein leads to activation of the other. A chain reaction is amplifying the system, but it also has for control to be implemented. When you have these coagula particles there is no control. It's like an out of hand. Everything gets activated all the time and everything gets consumed. So you have an immediate coagulation that used up all the anticoagulants in your system, and then there is no stopping of it. So what you end up with is this tiny little clots that are very highly pro inflammatory as well. And what they do, they go into your very small tiny blood vessels, the capillaries in your brain or wherever else you have capillaries and they block those. And what the blockage does is it induces strokes. Why did this happen? With this virus it's not very well known. In case of influenza, you can also have coagula particles and other very highly inflammatory situations. You will see that you can have these diffusions in the skin of the patients and you can have visible coagula particles, that transient and it will go away if you get better, but it's very difficult if not impossible to treat. And that's why you asked, what's the first hand? so just because I am included in the email list of the ICU clinicians They, it was, its really awful because, it's very frustrating There should we give them anti coagulants or should we promote coagulation or, you don't know how to interfere when a system is out of hand and everything is happening all at once instead of step by step. Q: In terms of getting back to work, are we going to be screening everyone for antibodies? What's your perspective as an immunologist? As an immunologist, definitely I think antibody screening might be a practical way of time to go about it but first you have to develop a screening systems that works so very good detection systems. I think they are more or less now available. But second you have to know who to screen, how you screen. You have to know how to interpret the immunoglobulin profile that you that you get from the patient. What does it mean if you have a ton of immunoglobulin? What does it mean if you have less immunoglobulin? Are you ramping it up or coming down or how long will immunoglobulin last in the circulation? I think we talked about that once. But I think that's still a viable way of going about it. Secondly, we have to maintain the physical distancing at least for a while. And people, I'm also on the task force, both, vice chancellors taskforce and the School of Medicine taskforce to work out the guidelines because we don't want everyone to be confused and not knowing what to do. It's much easier if it's reduced into a list of a few points that you can easily follow to protect yourself. It's still not that easy, but there is going to be a phase restoration and now because the number of positive cases is starting to wind down and also I think it was Sacramento County? Yeah Sacramento County that brought in some regulations that it's trying to loosen the lock down situation. So we are thinking very hard about how to get back to normal. So, for example, clinical work for obvious reason would need to proceed and maybe some parts of clinical research as well. Those are considered essential research and so those will be given the green light more easily than other types of works. Also we don't want the situation where all of a sudden everyone is back at work and it's party again and then there might be a possibility for cluster infections. And what we don't want to have is a situation where the ICU's would be overwhelmed and not be able to give you the proper care if you get sick because that would be really tragic. And I think authorities and hospital personnel are really highly concerned about that. So that's why it has to be step by step process. When will it happen? I don't now at the moment we are still in phase one and sheltering place is still in effect. So, I think just look out, read the news and just see what's going on for one thing, for second thing I think our vice chancellor is very up to date and he is very into it and he wants to inform the entire University. So, you don't have to be afraid that, Oh! shelter in place has been lifted and we didn't know about it for an entire week, it's not going to happen, you're going to know about it in the same hour once it is lifted.I th ink just follow the advice from authorities. That's the best way. And once these guidelines are released, I suggest to print them out or try to reduce them into very simple, very transparent, easily follow up points and make the door posters so that students, people who come in, would easily be able to see that. And that would also help prevention and avoidance of infection. Q: We know a lot of our healthcare workers have been exposed to COVID-19. Is there anyone tracking re-infection or whether the antibodies they might've generated are protective or not? Cause I think that's one of the things we'd all like to know. That's actually a question on a lot of people's mind and now I think just maybe the last recourse. We have such a testing availability for immunoglobulins that all healthcare workers can get tested freely and so that would actually inform us or inform everyone in terms whether you would know if you're being through it and your immune or if you get sick again, whether you're sick of the same thing. So as of now we don't know, I haven't seen any publications to this effect. Maybe some very few reports were immediately released to the media saying that someone got infected twice, but I am not sure if we can believe that. So you just have to check the literature for this because these kinds of studies are going on now for quite some time. And there was this publication mechanism I think it that are bioRxiV or something like that. It has three publication papers I posted. Sorry, I don't like to read too much non peer reviewed stuff because, who knows, and I don't want to confuse my poor mind. Sometimes science and nature papers get published in bio archives before they get published in those high impact Journals so it's worthwhile to look into it. Also, we have a very good Slack channel so I don't know if all of you guys are on it. If not, then I highly recommend that because it's full and full of such information daily and in fact it the reason I like it’s because people who are into specialty areas of research they predigests these things for you. So, there was one chain of emails or messages, either email or slack messages was reviewing a paper and you know, if I would have read it, I would have thought about, wow such an interesting study. And those who are the experts here at UC Davis, they demolished it. They said that it was a whole a boatload of crap. It was quite interesting. So that's another reason you should sign up on the Slack channel and sometimes go there and look for information there because they don't just read it, but they review this literature for you. So that's a good one. Q: Are you talking about the UCD COVID-19 slack channel for UC Davis? That's correct. UCD-COVID-19 on the UC Davis Slack. Not only UC Davis Slack, but there is a sub channel that's shared by other UC's, UC Berkeley and also the Bay viral consortium which is a big heavy weight consortium of virologists. You can go there and talk to them as well.
0 Comments
Your comment will be posted after it is approved.
Leave a Reply. |