 Dr. Samuel Díaz-Muñoz, a virologist assistant professor in the College of Biological Sciences and Dr. Brad Pollock, chairman of the Department of Public Health Sciences and Associate Dean of Public Health Sciences in the School of Medicine and the lead of the UC public health COVID-19 task force, opened the COVID-19 Town Halls providing us with information on the basics of COVID-19, the basics of viruses, public health issues, their perspective on the pandemic and more. The video of this town hall is available with English and Spanish subtitles here. Transcript of Dr. Díaz-Muñoz and Dr. Pollock's talks COVID-19 AND VIROLOGY BASICS Dr. Samuel Díaz-Muñoz, a virologist assistant professor in the College of Biological Sciences, was our first guest speaker. He helped set the pace for the rest of the town halls by providing a basic background of viruses and COVID-19. Below you will find some highlights from Dr. Díaz-Muñoz talk. Dr. Samuel Díaz-Muñoz talk So this is a scanning electron micrograph of a human hair. And if you compare that more or less to scale to bacteria that's popping down there. On your lower right corner. The hair is about 1000 microns thick across. The bacteria are about one microns across. The virus is about 1000 fold less than the hair. So you'd have to split the hair into 1000 pieces to get to the width of a virus, which is about 100 nanometers.  And from a genomic perspective, in terms of the virus genome size, we're talking about SARS CoV-2 the current circulating virus having a genome of about 30,000 base pairs. And these 30,000 base pairs compared to our 3 billion base pairs are very small physically. It is also a very sort of wimpy particle. It only takes about 70 degrees centigrade to actually inactivate this virus. This virus has a layer of fat, the envelope, a lipid envelope, and if you just use soap, you basically can just do away with that virus, it's inactivated, it can't infect anymore. UV will actually take the genome and mutate it such that it can't infect anymore. The human toll I pulled this up a couple of days ago, and you can see the number of confirmed cases are 750,000. Now today, it's up to 926,000, if I'm not mistaken, and this has a real human consequence, and we are losing people, people are dying in massive numbers. And I think it's getting to the point where people know someone that knows someone and/or they're celebrities dying so we can really all feel this pandemic maybe like not once before. How do viruses infect and their social interactions Viruses are organisms that are optimized to exploit biological interactions at many levels. The first level is the cell, they basically get in a cell and they are parasites, they completely depend on other organisms to reproduce, and they can be that small, they can afford to be that small because of that, because all they need is to have enough code, enough genetic code to hack that cell to drive the transcription and the replication of nucleic acids to be viral to make the cell into a virus producing machine. And then, at the end of that, you end up with massive amounts of virus. Okay, and I think this is the other reason how something can be so small and have such a big impact. Think about viruses as populations as swarms, some of their strengths comes from being in large populations. Now in the course of doing this of manipulating the cell into a viral factory, they destroy the cells. And that's one way we become sick. The other way we can become sick is that our own immune system will react and sometimes overreact to the damage being caused by the virus. And these are two ways that we can get sickness and death from the virus and then virus exploits the social interactions in another level, which is it exploits our own social interactions, this human necessity to have humans near to have a conversation to shake a hand, give a hug, give a kiss. The virus exploits that in order to move into the next host. And then it just spreads and the cycle keeps on going. Professor Brad Pollock is the chairman of the Department of Public Health Sciences and Associate Dean of Public Health Sciences in the School of Medicine. He is primarily by training and by career a cancer epidemiologist and biostatistician. Currently, he is the lead of the UC public health COVID-19 task force, which has assisted in setting policy in response to the pandemic. This includes moving students off campus, setting up a disease surveillance system for students and essential personnel who have to be on campus and modeling the epidemic so we can plan how we have to surge our hospital capacity. *Introduction above by Dr. Díaz-Muñoz Professor Brad Pollock’s talk About two and a half weeks ago, three weeks ago, the UC system wanted to organize a group of folks throughout the system that had some experience in public health to deal with this COVID-19 epidemic. I got asked to chair this committee and there's about 20 of us that are on it throughout the UC system. The first thing we were asked to do was to provide some guidance to the Chancellor's from all the campuses about what to do with the students. And our guidance was to get the students off campus, get them away, do social distancing, before anybody else was talking about this. And that's what got rolled out in a little bit about less than perfect pitch. But now, as of about a week and a half ago, all the campuses have students off as much as possible. Although some students have to remain on campus. Some of them are international students, they can't travel freely, others don't really have another home base to go to. So we're now concerned about the safety of students on campus. You know, for example, you have two students to a room, a dorm room. Well, that doesn't make sense. So we're writing and finishing up our guidance document right now about how to do the best social distancing we can on the campuses also had a surveillance for new cases, and how to cohort students, those that have infection, you know, we can put them in different residence halls, for example. We are working on some of those procedures right now and how to set up a permanent surveillance system that complements what the local county health departments do and what they're responsible for. Actually, at UC Irvine, some of our public health students down there are actually deputized by the Orange County Health Department. So they're actually officially able to collect private confidential data that's needed to survey for these kinds of diseases. So, other things to say real quick, what we can talk about all that today are some of the sort of interesting things that are popping up now. And all I can tell you is those of us that have gotten dragged into this. It's been total adrenaline, there's been no sleep. This is one of the few times in my life where the work that I do doesn't have a payoff 20 or 30 years from now, I do cancer prevention work. So if we tell somebody to not smoke cigarettes today maybe you'll see an impact 30 or 40 years down the line, this is the first time in my life that what we do is actually having an impact on people's lives you know in trying to prevent more death and more morbidity now. All right, so now you should be able to see this UC Davis Health novel Coronavirus. So this is an example though of trying to keep track of statistics as the Epidemic is raging. 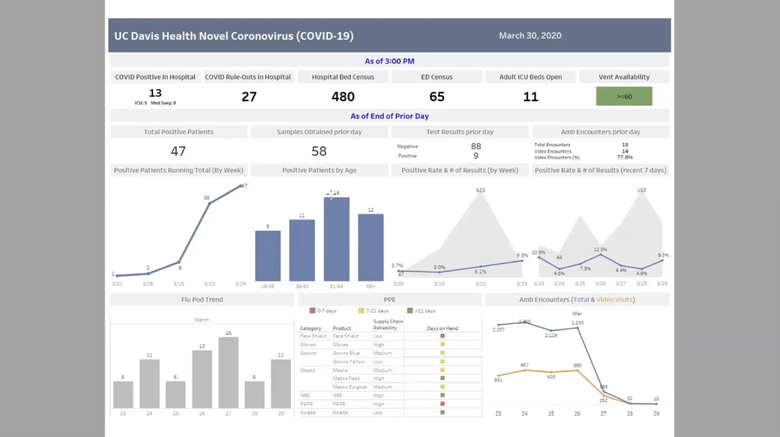 This CHIME application was developed at University of Pennsylvania here where you can plug in information about your regional population, and then look at for the particular hospital, what's their market share, and then look at the current number of hospitalized patients with the infection. And then you put in some other parameters like doubling time and so on. When you do this on the right hand side, you're actually seeing projections now, based on this, if I go ahead and say the doubling time goes down like this I'm lowering it down, you see this is the epidemic curve is shifting. This is the doubling time, the time for the number of cases to double. So you can see interactively, how that affects this epidemic curve. That's one model. *Reference for CHIME: https://oto.med.upenn.edu/2020/03/31/covid-19-hospital-impact-model-for-epidemics-chime/ 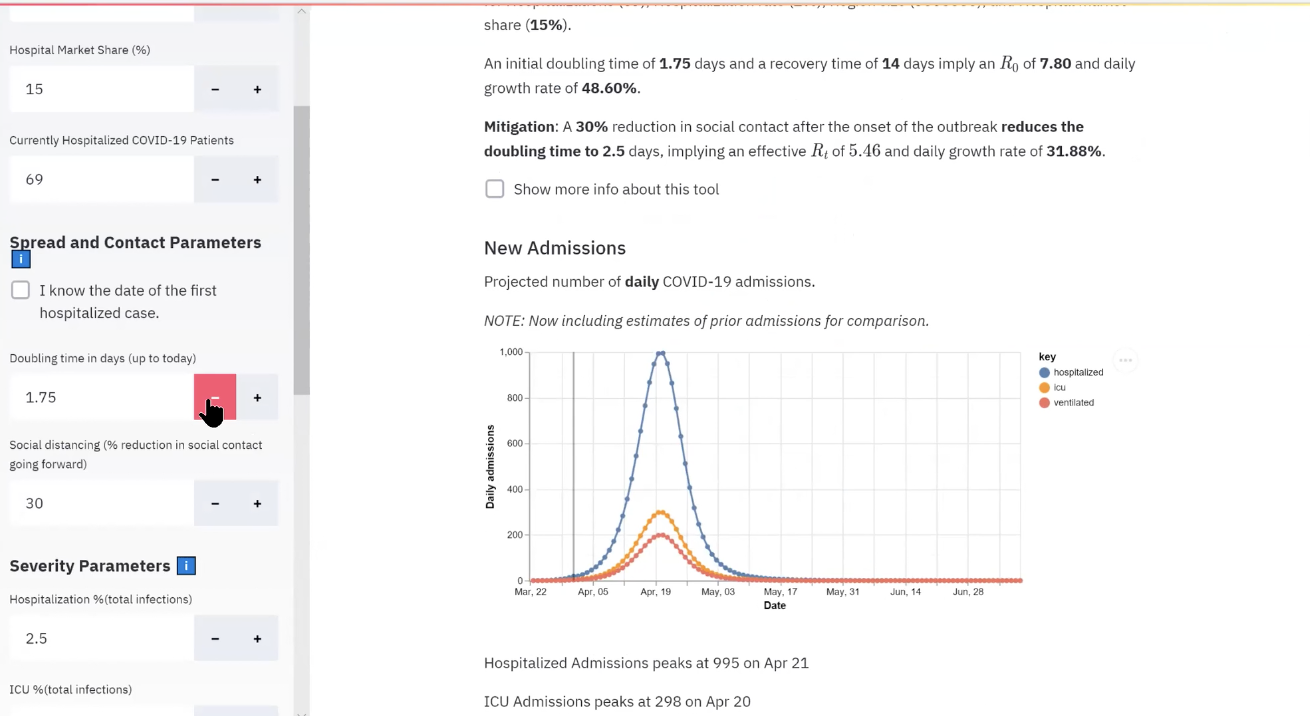 The other model here that was put out by the Gates Foundation funds University of Washington, and they have the Institute for Health Metrics Evaluation (IHME). They have a calculator that's out right now. And I pulled up the data for California. And I'll just show you the way this works is at any point along the axis here, this is based on a predictive model. If you go to April one, right now it's predicting that we have in the state of California 26,000 beds available, ones are needed right now only 4,000. That's good. The number of ICU beds is about 2,000. The ones we need right now are 780. So as you sweep through this, you can kind of see what happens. These numbers change as you move the epidemic out. If we get to the end of April, for example, let's go right over here to April 30. There we go 29th. That's good enough every 30 so you're looking at you can kind of get an idea of what the surge capacity is going to be now, you know, in New York City right now, New York, they started doing some of these efforts to do social distancing. After the epidemic was really brewing and you're seeing what's going on now, they've stripped out their bed capacity. And they're at the capacity now of not having enough ventilators for people. So now you're getting bioethicists involved in deciding who should have access to ventilators on ethical basis, I mean, that I don't want to get to that, hopefully we won't in California, we did implement these social distance measures. *Reference for Health Metrics Evaluation: http://www.healthdata.org/ 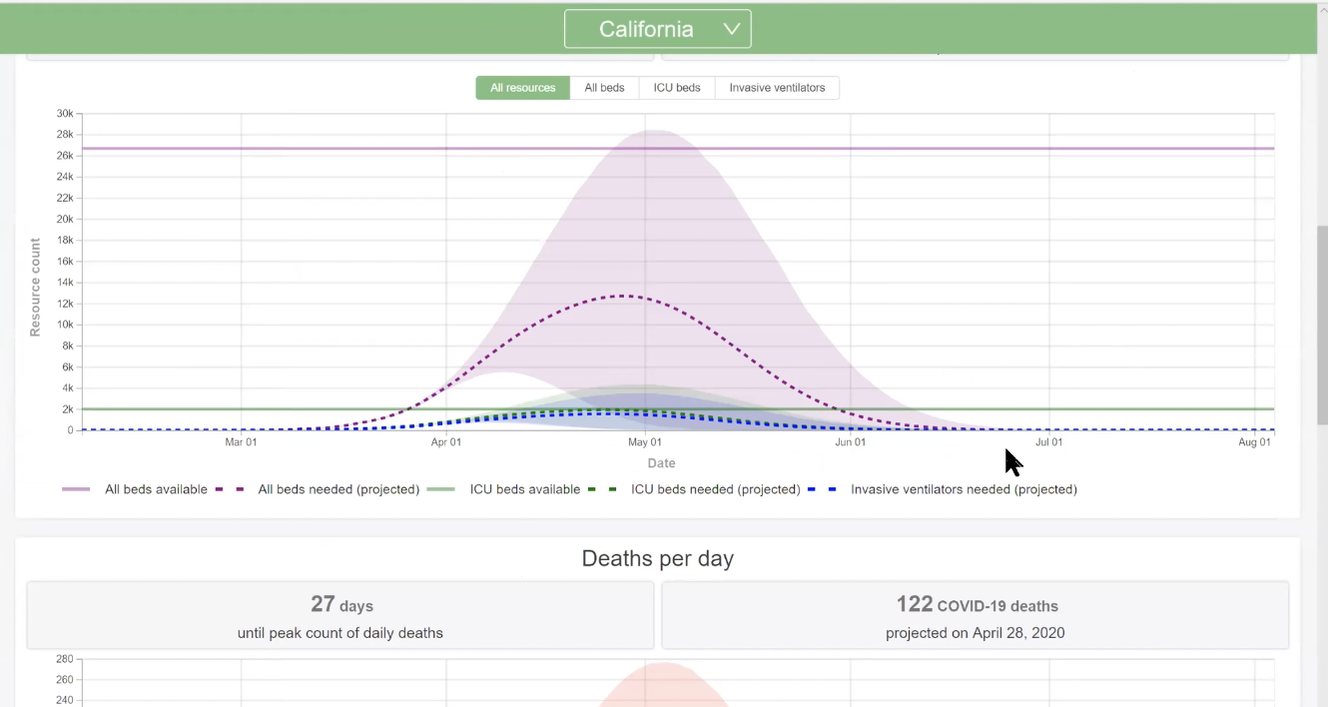 You know, it could have happened a week earlier, but it did happen now. And we think there's going to be a pretty dramatic effect, at least at drawing out the length of this epidemic. When you do that. They call it flattening the curve, you're moving the right side out a little bit more, you're doing that for the purpose of hopefully keeping the surge numbers down and then when you have a lower number at any one time so that your hospital systems can keep up with that demand. So That's just an example of something and there's a couple other ones, people put out some calculators. I think the question I'd ask people to think about is how do you handle a challenge like this? This is a huge challenge. We've never had anything like this before. In my lifetime we've had it back in 1918. There was the flu epidemic then the pandemic and it killed millions of people back then. These times are different now. But how do you handle this? If you think about the problem, you have to think about it from all levels. I really started out as a biologist, I still think my bones are being a biologist. I've managed to bring that into public health. Some people in public health start as folks that do sociology, behavioral work. And so they come at it a slightly different angle. But I really think that if you think about problems like this, you need to have challenges at the level of basic science. What's going on molecular way from a cell standpoint, even from sequences for DNA, RNA. You think about it from a clinical standpoint, we have patients, physicians are seeing these people. How do you do the diagnostic tests? How do you figure out whether the tests are working properly? Do we have enough distribution of tests that's kind of in the clinical realm, and the other realm is the role of public health is really looking at the population base and these are not really separated? Those of us who do epidemiology we move to doing molecular epidemiology, genetic epidemiology 25 years ago, I mean, right now, I don't think you can be a good epidemiologist without having a very strong biological background. That wasn't true when I started Graduate School in 1979. If I came in as a sociologist doing surveys research, I would have been much better off all that biology I learned wasn't useful until the AIDS epidemic yet. So, you know, things have changed a lot. Last things I'll leave you with before we open it up here is some of the the offshoots of this epidemic are really kind of social in nature. So think about this. We have a shelter in place orders going on right now. What about vulnerable populations? What about people who can't take care of themselves, people with illnesses and predispositions and disabilities, those they can't conduct their activities of daily living. We've got workers who have to go into their homes, there's more of a risk for them being exposed. I'll tell you what I did Last week. I got an email from the Sacramento County District Attorney. They asked me if I would help them with some expert work and testify to try to get the Sacramento County jails thinned out so that they can actually put the inmates at lower risk by getting rid of some of the people in the jail and I ended up they were gonna pay me to do this, and I said, are you kidding? This is pro bono work. So I actually wrote up an affidavit essentially talking about what the dangers are of keeping prisoners in very crowded conditions. So they actually let out 400 prisoners from the two prisons that Sacramento County has on the basis of public health considerations for risk and so on. And yeah, of course, there's balancing risks off, but these were the lower risk prisoners or people that were incarcerated. So that was kind of a thing I didn't expect to do. And then the other thing we just talked about before we officially started the class, what about what do we do next? The epidemic is going to peak and it's gonna start coming down. And what do we do? When do we know it's safe? How do we go about getting back to life, it will end we know that unlike some other sorts of things that have happened before. This is something that is going to be moderately affecting us in large numbers and with high severity. But when we come down off this thing here, what do you do? I'm over 60 I'm 63 I'm vulnerable. until they get a vaccine where I have some protection. Am I gonna go and circulate as I did before shake everybody's hands and go to board meetings? Everything else? I don't know. So they're working on immunizations. Now that vaccination, they're working on treatment for people that do end up getting sick, are there things we can do. And the treatments are likely to be discovered a little bit faster, probably within six months or so we may see some good efficacy studies for people that are kind of severely ill, perhaps to keep them out of the ICU and from dying on the ventilators. But that's not good. And I just want to point out to everybody here, that you've heard that this virus here affects everybody it does. The first warnings that we had from a public health perspective were let's make sure we protect the vulnerable those that are elderly with underlying conditions. But think about this. You've heard about cases now of folks in their 20s and 30s dying. It doesn't discriminate. There are people that get very sick. I have a few friends that are positive and are now going through it and It's not something you want to have, you are less likely to end up dead if you're younger and in good health. But there's enough of a risk there where I wouldn't wanna take a one in 200 chance that, you know, to die from a bug like this. So it's a very, very serious thing. Transcript of student questions and highlights
Q: Viruses need hosts? Where do they come from? How do they evolve? Dr. Díaz-Muñoz-The short answer is we don't know. The longer answer is, they were probably there in some form, from when life was getting started. So there are basically ways..., in the course of evolution of life, there's always been a way to game the system, and a way to get a free ride and space for parasites. And so they were probably in there from the very beginning, probably in a very, very different form. But that's a great question and I can definitely dig into that more during my module. Host- I'll put now that the radio lab podcast takes the opposite view that maybe viruses simplified from more complex cells, at least with mega viruses, so it's an interesting alternative view about where viruses might have come from. Q: Is this just a very fast moving disease? Or is there something different about it from an immunological perspective and how our bodies adapt to it? Dr. Pollock- Well, it is novel. I mean, I think that's the key. You see the prefix is novel Coronavirus. We have Coronavirus is that's one of the more common causes of common colds. They're very ubiquitous. This is a novel virus, which means that nobody has natural immunity to this. And that's what makes this so difficult because there aren't the typical tools that we have available to us that allow for some protection. Dr. Díaz-Muñoz- The SARS like Coronaviruses, is a group of beta Coronaviruses. Their reservoir species are bats as a group so that's sort of what we think is the quote “natural host” of Corona viruses. And then what happens is these SARS, like Corona viruses after the SARS, the first SARS outbreak in 2002-2003, people started researching them and saying wait, what's going on with these Corona viruses in the bats? and there are 500 identified Coronavirus, different Corona viruses in bats. Bats in general do have a lot of viruses, but the important point for them in this epidemic is that the home of Corona viruses, or at least that the SARS like Corona viruses is our bats. Now what happens is it turns out that many of these Corona viruses can actually infect humans without changing at all, right? They can, we have the receptors that they can use to enter into us and other mammals. So that makes it really easy for them to jump. And in fact, there were some studies showing basically that at least in cell culture, and with humanized mouse models, several of these SARS like Corona viruses could infect humans. So we knew that, you know, this was a possibility. So I just want to put that out there. When someone says no one saw this coming. There were many studies that people who were studying this and paying attention knew that that was a probable thing. And what happens then that's where the immune part comes in. And sometimes in this human jump, there's an intermediate host. So we know for SARS one it was feline carnivores called civets, in the case of MERS Middle East Respiratory Syndrome it was camels. So sometimes you have an intermediate host that jumps in we're not completely sure what's happened yet with the current SARS CoV2 too, but we'll find it. Q: Are there multiple strains of this particular Coronavirus out? There people that are pointing to Italy and saying that must be different. Can you guys shed a little bit of light on that? I think people are super interested and worried about that idea. Dr. Pollock-The case that we had at UC Davis Medical Center that was this community acquired case, it matched up with a Wuhan virus sequencing. So it was I mean, there's no question that's where it came from, but I don't know the level of variability. Dr. Díaz-Muñoz- This is a really interesting question. Right now most virologists, pretty much all virologists would not say there are a bunch of different strains running around. In fact, what's striking about this outbreak is how little change has happened with this virus. And remember that I told you that this virus can come into humans no problem, right? No mutations, it doesn't need a special mutation. So it just came in. And as Professor Pollock said, all the strains that are circulating now that we've sequenced lineup perfectly with the Wuhan Coronavirus, so we know it was a single origin. And if you look at the diversification, the mutations that have accumulated because this is a microorganism, and it replicates quickly, so you do have mutations. So this is like bacteria, if you're familiar with that, but even faster, those mutations that are happening are happening and our clusters geographically. So it served as a sort of time clock. But the important part is they don't correlate with a particular disease state or a particular immune response right now. And those are part of the things that would identify different strains. So in influenza, for example, we use the structure of the immune sites, to classify them into subtypes, and then strains, or there's a particular level of sequence divergence after which we say, okay, this is a different strain. This is not the case. Also, this is an RNA virus. The genome is composed of RNA. Usually, organisms with RNA viruses, with RNA genomes, mutate very quickly because the RNA polymerase doesn't have a repair system. Normally, it doesn't have what's called proofreading. This Coronavirus has proofreading, it can repair mutations, so it is actually exceptionally stable. So that's something to keep an eye on. I'm hopeful that that actually means that once we find a treatment, rather a vaccine, that it actually will make it so that it sticks. Q: How similar is this to the Spanish Flu 1917-18 pandemic that occurred? Are there gonna be similar trends in terms of epidemiology? What actually caused that influenza to burn out during that period of time? Because I don't think I know the answer to that. So maybe you guys can start giving us some historical perspective. Dr. Pollock- I think St. Louis was an example where they did the social distancing stuff, they did the shelter in place business, and it showed these dramatic differences in terms of economic recovery, the death rate, mortality rate as well as economic recovery. Turns out when you did this study Public Health measure to separate people. While it slows down business right away. It showed that the economic recovery after the end of the epidemic was much, much faster. The other thing is our knowledge of biology and the ability to do things in greater orders of magnitude right now, for example, diagnostics. So, you know, even though we haven't had a widespread, enough availability, diagnostic testing is ramping up very quickly right now. The hospital went from being able to do 20 tests a day over at UC Davis, to now 200 a day and it'll be ramped up to 6000 a day, probably within a month. The idea of developing therapeutics, even developing a vaccine right now, I don't know how many years it took before we developed some vaccines for influenza, which are variably effective based on the strains that year and so on. But you know, we're talking about years before, we're now talking about vaccine development in the space of 18 to 24 months! And that's, and most of that wait time is really the clinical responses. You can't go so fast looking at human beings, and seeing what the responses are both from a safety standpoint and efficacy, but just the knowledge that we have about the biology has driven things at a much cheaper rate. And again, they are two separate bugs. *Reference for St. Louis cases: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2862338/ Dr. Díaz-Muñoz- Yeah, I would jump off of the two separate bugs, comment. So I think when I talked about the emergence of this virus from bats using an intermediate host or not, with influenza, it's very, very different. So the emergence is from birds. And those strains actually are not very good at transmitting between humans so they can’t get into us. And they're very, very pathogenic. And so when they get into us, they kill us. But then they can't really spread to different hosts. They can't unless they happen to exchange genes with a human flu virus. And that's usually what sparks pandemics. And that's why in swine flu an intermediate host, an intermediate host for an avian strain, then exchanged genes with a mammalian strain all of a sudden to gain the ability to spread quickly from person to person. So in that origin, it's very different and it mutates very quickly. There are other things going on in the influenza pandemic, too. There were basically co infections with bacterial diseases, people will get bacterial diseases that were worse. There is that, what the impact of that has been it's hard to sort out a century later. But there is some evidence that that happened too. So everything was different sort of the communications, the treatments, all of that was very different. Dr. Pollock- World War One, trench warfare didn't help. It's apples and oranges. But we talked about interactivity. So clearly, Sam just gave you a good example of sort of how easy it is to transmit across species. If we just think about different bugs that we have, you know, you remember about three weeks ago, people were very worried there was a New England Journal of Medicine article that came out that showed that they were able to aerosilize this virus COVID-19 and suspend the virus in a stable state at least for at least three hours and aerosol that got people extremely worried that was a multi step, multi institutional study including some folks at UCLA. I saw it and we said, Oh my god, you know, people are gonna go nuts because now they're gonna worry that it is airborne, if this were a real airborne virus, the implications would have been that we would have effectively had at least less than half of the available ICU beds. Because our ICU do not have that level of airflow control, they have hepa filters, but they would have had to have something if it was something like measles, which has a much higher infectivity rate they talked about R naught, which is the the number of people affected from one case on the average. And with measles, it's airborne, is a very small particle. So you have R naught in the range of 20 to 30. This bug is considered to have an R naught of two to three and a half or something in that range, an order of magnitude lower. So that's a very important consideration also is that every bug has different characteristics in terms of sort of the mode of spread and as well as the physical nature of the bug itself and its stability. So we worry about that a lot. But these characteristics do distinguish the patterns of occurrence and populations. That's why you see these different epidemics. Q: Corona virus could become seasonal? We might kill it over the summer and then it comes back in the fall? Dr. Pollock- We were looking at Australia, New Zealand very carefully, right there, they have the opposite seasons here. They saw no real impact on the epidemic curves from the seasonality looking at the southern hemisphere. We do know that the virus is not as stable when it's warm out. So if you talk about the virus getting on to hard surfaces, contact surfaces. In warm climates, the virus probably has a lower half life, but we're not seeing the typical Corona seasonal patterns based on what we see in this hemisphere. Dr. Díaz-Muñoz- Correct, so I want to chime in on that. Yeah. I heard Mark Denison, who's a professor at Vanderbilt University who studies Corona viruses, say that viruses are not seasonal. They're migratory, right? And so in influenza, we actually exploit that. And we look at what's happening in the different hemispheres. So we can try to predict which strain to design the vaccine against. And so Professor Pollock hit it right on the head, all you have to do is look at warmer climates. We have it in the tropics, spreading right now and increasing. We have it in the opposite hemisphere, where it's the opposite season, and it's still spreading. So I would like to believe that but it doesn't look like that's necessarily gonna be the case. *Reference for Dr. Denison’s video: https://www.youtube.com/watch?v=wZVbbag1ztI Q: A bunch of questions were ranging around the idea of what kinds of treatments would be the fastest, the best. I know, antivirals have had incredible success lately in a whole class of viruses. So could you maybe share your thoughts on what is the best strategy moving forward? Dr. Pollock- Well, the best strategy would find a drug on the shelf that has been safety tested and would be effective for this and so that's exactly what Gilead is doing now with their antiviral and it was actually designed with some thought of Coronavirus, but really deployed for the Ebola epidemic, not super effective for Ebola. But they went ahead and with this novel virus, this is the clinical trial the Chinese started about three and a half weeks ago. In the states two weeks ago this trial, Gilead trial opened up and there's 60 sites now where it's being done including UC Davis Medical Center. So the best thing would be, we have a super effective treatment on the shelf that works against the new novel bug, that would be the best thing. Even better than that we have a vaccine that would confer some immunity, but we don't. Then the other thing to think about is, when do you administer those treatments? Is it done when they first developed symptoms? The other treatments that we're trying right now, I know in China it started about a month and a half ago, it's conservative. They conserve sera so they actually were looking at antibodies from people who recovered from the disease. We are now starting those trials in this country. I think the trial that I saw to use passive antibodies requires that people that are recovered have pretty high titers, antibody titers for this COVID-19. We're trying those trials right now. They're just starting up again. And those are being aimed at people that are just going into ICU at that stage of their disease. So that just, I mean, there's a lot of other things going on. There's drugs now that have been on the shelf to look at acute respiratory distress syndrome (ARDS). That's the very final stage. If you develop pneumonia, you're on a ventilator. The ARDS is kind of the final stage there. There are drugs that have been developed for that that aren't super effective, but we're looking at those now to prevent you from dying. If you are in the ventilator, you kind of go downhill. Final thought Having biologists as emissaries for public policy in general is so important and it's my wish for every student listening that you seriously consider taking the expertise you're gaining here and in your major and using it in that way, right. You don't have to just see patients in the clinic.
3 Comments
8/25/2020 11:59:46 pm
arrondisement, Paris. Image posted to Facebook by the artists (image in the public domain) 2/14/2021 12:03:08 am
SUMO Digital Scale produces health scales, for example, baby scale, bathroom scale. There are assorted health scales going from 20 kg to 200 kg having correctnesses 10 g to 100 g. Course of action is done unequivocally in own plant. The highlights are magnificent LCD show, inborn long fortress AAA battery, High accuracy Load Cell, 150% over-inconvenience assurance framework, extreme development verification game plan. To see significantly more if it's not all that amount trouble, reach us or visit our site. Your comment will be posted after it is approved.
Leave a Reply. |